
The people's voice of reason
The people's voice of reason
Yes, as an adult I think it is an important document to address the possibility of imminent death when you are no longer able to communicate your health care in certain circumstances.
A Living Will in addition to the naming of a health care proxy make up two documents that can function independently but collectively are part of a document called an “Advance Directive for Health Care”. The first component is the Living Will. The Living Will states that you are an adult (at least age nineteen in Alabama), have an understanding of what these directions mean and that you want your family, doctors and health care workers to follow them. Furthermore that you can void the document by tearing it up after signing a new document or tear it up and have another person nineteen or over write your wishes down.
The document defines what life sustaining treatment in a terminal illness or injury is, such as medicines and machines that will keep you alive but not cure you. The Living Will first asks if you want life sustaining treatment which is answered by initialing beside a “yes” or “no”. The next set of questions asks whether you want artificially provided food and hydration which would be through a feeding tube or an IV. Placing your initials next to the “yes” or “no” is the correct way to respond. When one considers the question you realize does this mean I want to be starved to death or not be given fluids that may result in my death? The truth is yes, but there is a balance. Imagine lying in a hospital bed unable to communicate and your doctor and another doctor have determined you will likely die in the near future. If you are given food and hydration it will somewhat delay your death but not heal you. Several years ago a local physician who headed palliative care at a local hospital discussed that very subject with the Alabama State Bar Elder Law Section. It was his understanding that withholding food and hydration created a sort of euphoria for the patient and not that feeling of really starving to death. You should discuss those medical aspects with your personal physician; don’t take any medical advice from this and for that matter unless you come to see me as a client don’t even take the legal facts as gospel from this article. Everyone has their own situation.
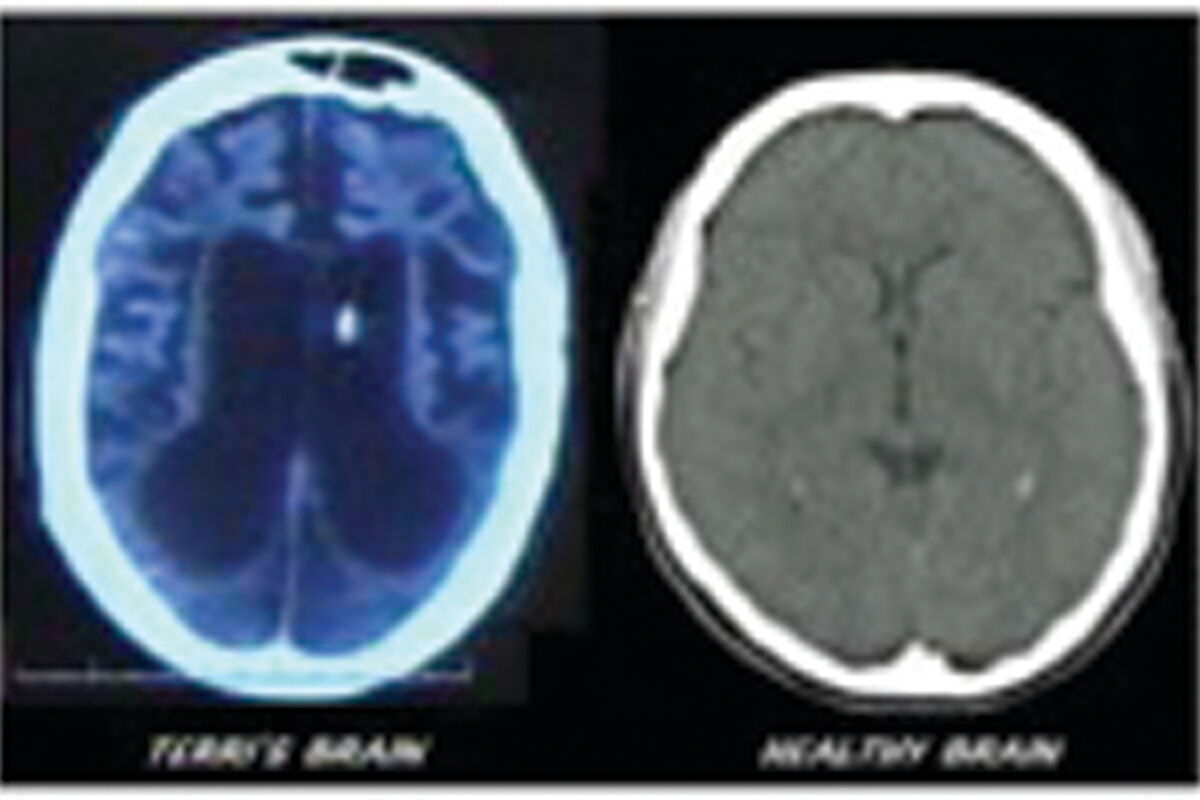
The second aspect of the Living Will is the same set of questions for the permanently unconscious state (some refer to as being in a permanent vegetative state). The difference in criteria is that your doctor and another doctor familiar with this type of condition (such as a neurologist) make the determination that you will likely die in the near future and again you cannot communicate your wishes. This situation makes me think about the Terri Schiavo situation out of Florida. Note the two CT scans from the internet, one of which is said to be that of Terri Schiavo which was supposed to have been released by Dr. Ron Cranston, MD.
If the internet depiction is true, then one can note the small lateral ventricles of the healthy brain and definitely see that hers are greatly enlarged and a reasonable person would believe this to be a very unhealthy brain. Terri’s husband went on to live with another woman following Terri’s fall into the state that she was in. I remember seeing her on television and recalling that her eyes were open (though I understand she was then blind). She certainly seemed to lack awareness of life around her but I don’t know if one considered her unconscious. It became a national court case as her “husband” related a conversation that he and Terri had where she stated she would not want to live if in a state such as she became. Her parents argued that she should continue to be kept alive. The Court sided with Terri’s husband and she was allowed to die less than two weeks later.
The second section is where a proxy can be named to make health care decisions and can function as a separate document without having a Living Will or it can be used in conjunction with the Living Will. Anyone named as a proxy are given several powers needed for health situations which includes the necessary rights under HIPAA. The first set of questions ask whether you want to name a proxy which is basically a power of attorney for those purposes and then whether you want the proxy to make your decisions found in the Living Will or work in conjunction with your Living Will to make decisions not covered by the Living Will. I don’t find death to be black and white in nature and different variables may arise that needs someone to decide upon. You name a primary person and a successor should the primary not be able to make any decisions. Having a person that can make these decisions if necessary take some thought and discussion. Regardless, it can be very difficult when it comes down to it.
In some ways it all seems a bit brutal. It is not a Dr. Kevorkian action The Advance Directive is addressed under the Alabama Natural Death Act. In a world where life may be sustained by medicines and machines for some time when one may have no awareness of being alive, this document seeks to allow people a more dignified death that may have been experienced one hundred or more years ago. I recall reading about a relative from the 1800’s who left church upon feeling ill and sat under a tree somewhere outside the church. When reached by those checking on him said that he “was in the throes of death”. There were no machines, medicines or procedures to cure what I perceived as a heart attack.
I use a form that was cobbled together by the Alabama Medical Association and the Alabama State Bar. It’s a way that individuals can predetermine their own course of death should the end come to that.
When it comes to it I have learned partly from personal experience. When my mom fell and hit her head there was no Advance Directive to consider because she did not want to fill out the document. It was clear to my Dad and I that Mom could not survive. In the absence of an Advance Directive, the next of kin are queried on what to do or not to do. When my dad’s health was declining after he broke his hip last year I was told the “decision” may have to be made. Regardless of everything it was not a decision I ever wanted to have to make as named primary proxy and fortunately I did not.
A “Do Not Resuscitate” (DNR) is different and separate than an Advance Directive. One that is in fragile health may not be resuscitated should they suffer a cardiac arrest. An elderly person in otherwise fair health and having vitality in life may have a DNR as resuscitation is rather violent and cardiac compressions can fracture multiple bones.
Consider an Advance Directive for Health Care and talk to your family about your choices. The family member that comes in when you are close to death may contest your choices and cause an uncomfortable delay in an unavoidable natural death. Make sure all close family understands and more importantly respects your decisions.
This article is informative only and not meant to be all inclusive. Additionally this article does not serve as legal advice to the reader and does not constitute an attorney- client relationship. The reader should seek counsel from their attorney should any questions exist.
“No representation is made that the quality of legal services performed is greater than the quality of legal services performed by other lawyers.”



Reader Comments(0)